| Home | Contact Us | Site Map | Search |
|
|
||||
|
|
|
|
|
| |
||
|
This file is provided for reference purposes only. It was current when it was produced, but it is no longer maintained and may now be out of date. Persons with disabilities having difficulty accessing information may contact us for assistance. For reliable, current information on this and other health topics, we recommend consulting the NIH Clinical Center at http://www.cc.nih.gov/.

|
||
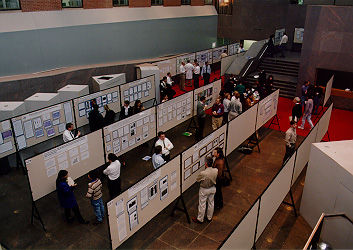
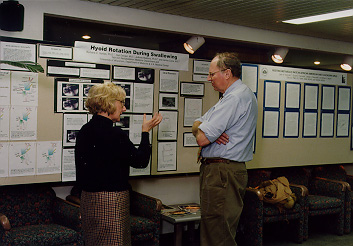
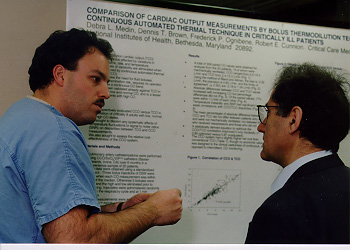
PosteringPosters sessions during the Feb. 10 Clinical Research Day offered the NIH community a chance to look over and talk about the science. Dr. Harold Varmus, NIH director, kicked off the event by reading a letter to attendees from Maryland Senator Barbara Mikulski: "As you fight the battle to prevent illness and cure diseases, know that I will fight just as hard for your long-term funding."in this issue:Clinical Research Day spotlights work across NIHNIH celebrates clinical researchCreativity, energy keys to clinical research engineScience, designing a building find common groundCC storehouse valuable in hepatitis huntFrom the directorWorkingbriefs:
Clinical Research Day spotlights work across NIHFaced with pressures and promise, clinical research is at an important crossroad. "We are all aware of the pressures that exist in clinical research here and around the country," Dr. Harold Varmus, NIH director, told those attending NIH Clinical Research Day here Feb. 10. "Pressures generated by shortage of funds, by managed care, by the long-term responsibilities and debts of going into clinical research. We feel all these tensions at a time when we recognize that the fruits of medical research that seem so tantalizing as a consequence of remarkable advances in molecular biology and many other forms of laboratory science should be generating great advances that have specific benefit for patient care." Those forces provided a genesis for the gathering of NIH scientists to, Dr. Varmus added, sketch out a longitudinal survey of the clinical research done in the NIH intramural program. "It is in that context and with the prospect of having a great new clinical research center building and given our sense of responsibility to make that the best possible place we can that we thought it would be useful to spend the day together." A strong enterprise for clinical research nationally and at NIH is a constant reminder to all medical scientists, he noted, of the ultimate purpose of much of scientific work in this country-to help patients. "The patient and investigator are engaged in unusual interaction," Dr. Varmus pointed out, "one that we hope will lead to benefit to each other and to society." It is, he added, a relationship that entails risks, especially for the patient who may not benefit from the research. "Those are risks that we need to consider seriously and thank our patients for assuming." Clinical research is subject to the same critical thinking as any other phase of science, he said. "There is clinical and patient-oriented research that is good and some that is not so good. Things that create new paradigms and things that are repetitive. Excellence is what we're after." The Clinical Center, with revitalization efforts under way and new construction coming soon, will provide an important hub for that excellence. "Our challenge is to utilize today's technology to establish the best patient-care environment for doing clinical research," noted Dr. John Gallin, CC director and NIH associate director for clinical research. "To develop the proper infrastructure to harness the computer age, to facilitate patient access to clinical investigators, and to provide the infrastructure to enable clinical investigators to conduct their science with minimal administrative or regulatory burdens." Education and access are crucial to the future of clinical research. "A new program to train medical students that was recommended by the [NIH director's] Panel on Clinical Research will be initiated this year," he said, adding that the pilot, under the leadership of Dr. Michael Gottesman, NIH deputy director for intramural research, will bring third-year medical students to NIH this summer to learn about clinical investigation. "We would like to open the doors of the Clinical Center to the extramural investigators to promote more collaboration with intramural scientists and to give extramural scientists access to some of the special resources at the Clinical Center," he said. "My goal is for every Clinical investigator in the world to spend time at the NIH Clinical Center, whether for training, a long-term career, collaboration, or for utilization of special resources," Dr. Gallin said. "My goal is that every patient with a medical problem will know about the Clinical Center and turn to NIH for advice and, when appropriate, participation in an NIH protocol somewhere in the United States. Our challenge for the future is to constantly adapt our infrastructure to meet the demands of both patient care and clinical investigators." (by Sara Byars) NIH celebrates clinical researchNIH's first Clinical Research Day, held on Feb. 10, drew the curious to its scientific presentations, workshops, and poster presentation. It was an event designed to celebrate the history of clinical research at NIH and, more importantly, the future of clinical research here.
 Creativity, energy keys to clinical research engineDr. Harold Varmus, NIH director, called on clinical researchers to inject creativity and energy into the research community. Referring to the long-standing tradition of scientific achievement at NIH, he touched on categories of change that can pave the way for that revitalization. In his Feb. 10 talk on the future of clinical research, he described one NIH initiative that introduces a standing committee representing the best clinical investigators from the institutes. The researchers will meet regularly to think and talk about clinical research, find the holes in the programs that need to be filled, and-through dialog-create an atmosphere of creativity and excitement for novel treatments and approaches to clinical problems, he said. "More attention should be paid to visionary thinking, to clinical research as a central activity on this campus," Dr. Varmus said. Training initiatives offer another key to the future, Dr. Varmus noted. The popular Core Course in Clinical Research will be expanded, with new content that will "make it clear that clinical research is a science with rules and demands of its own." With a nod to the recent accomplishments in neuroimaging, gene transfer, and molecular genetics, he outlined plans for a new training program in clinical research for medical students. "Interest in this program is high. There are already 75 applications for this new program after a single pass of advertisements to medical schools," Dr. Varmus said. As another way to inject more training opportunities and interaction between junior and senior staff in clinical research, Dr. Varmus suggested an on-campus Ph.D. program that would allow students to gain exposure to some of the clinical problems that most students are unaware of. Dr. Varmus noted he has met many students who are interested, for instance, in how bone is influenced by mutations in genes and yet are unaware of the clinical potential of using what is studied in the laboratory to understand diseases like osteoporosis. "Researchers who do not have exposure to patients could gain a lot from sitting in a room with a patient, learning about a specific disease to energize the research they later do at the bench," he said. All the upcoming changes-and other changes yet in discussion-are aimed at achieving the greatness Dr. Varmus foresees for biomedical research conducted in the new Mark O. Hatfield Clinical Research Center. "I hope today's exercise will help focus attention on the things we can do as a community to enrich our clinical experience and productivity." (by Laura Bradbard)  Science, designing a building find common groundThe formula for designing a good building is much like the recipe for good science. Tons of work. Trial and error. No shortcuts. Fundamental knowledge is required, but so's a large dose of intuition. And, Robert Frasca told the Clinical Research Day audience, "It's important to know when you're coming to a dead end." Frasca's the partner in charge of design for Zimmer Gunsel Frasca Partnership, the firm designing the new Clinical Research Center. "We really believe that a good science building can contribute to good science," he said. "In designing this building, it is a partnership. We literally learn from one another. The more emotional investment you have in the building, the better building it's going to be." To that end, the design team has spent months interviewing CC and NIH staffers about what they need and want in a building. Some design considerations so far:
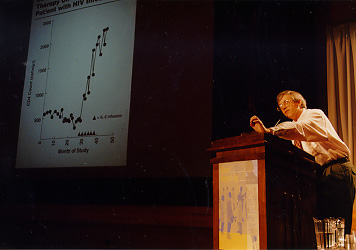
 CC storehouse valuable in hepatitis huntIn one of Clinical Research Day's seven scientific presentations, Dr. Harvey Alter, chief of the infectious diseases section in the Department of Transfusion Medicine, highlighted the value of the Clinical Center's rich storehouse of blood samples in the hunt for hepatitis viruses. The CC's Transfusion Medicine Department began collecting serial pre- and post-transfusion blood samples from open-heart-surgery patients and from donors in the early 1960s, after the discovery of the Australia antigen, later named hepatitis B surface antigen. "Before 1970, the incidence of post-transfusion hepatitis exceeded 30 percent in our open-heart-surgery patients," said Dr. Alter. "In 1970, we switched from a partial paid-donor system to an all-volunteer donor system and began testing for hepatitis B. This reduced the incidence by 80 percent to a residual rate of 12 percent." But what caused the remaining cases? In 1973, here at NIH, NIAID researchers discovered the hepatitis A virus (HAV). "We immediately tested our stored blood samples and found that not a single one was due to HAV." The mystery agent was called non-A, non-B hepatitis until 1989, when the Chiron Corporation cloned the hepatitis C (HCV) virus. "Again we tested our stored samples and showed that the agent Chiron had cloned indeed accounted for 90 percent of non-A, non-B hepatitis cases," said Dr. Alter. In 1990, a test for HCV became available, further securing the blood supply, and in 1992 a more sensitive test was introduced. "We have closely followed 650 blood recipients since then, and not a single one has developed hepatitis C," said Dr. Alter. "If testing were not in place we would have expected 30 cases in this size population." In the past year, the Clinical Center's stored samples have been studied for the presence of the newly discovered hepatitis G virus (HGV), which was thought to account for the 10 percent of posttransfusion hepatitis cases that are still unexplained. Although about 1.5 percent of volunteer blood donors are positive for this agent, a rate fivefold that of HCV, HGV appears not to cause significant illness, and may ultimately prove not to be a hepatitis virus after all, according to Dr. Alter. As the search for viral causes of hepatitis continues, says Dr. Alter, the Clinical Center's stored blood samples will no doubt be called into service once again. (by Sue Kendall) from the directorby Dr. John I. Gallin, CC director Ever wonder why we do the things we do? In an organization as complex as ours, it's an important question. We have to define who we are, where we are headed, and what we must accomplish to get there. Traditionally, these elements are called mission, vision, and long-range goals. Think of them as a foundation on which we build. Our strategic plan is the blueprint. The Clinical Center's Board of Governors gave their stamp of approval to ours on Feb. 10. The first brick in that foundation defines our fundamental purpose, our mission: The Clinical Center is the clinical research facility of NIH. As a national resource, it provides the protocol-specific patient care, services, training, and environment needed to initiate and support the clinical research sponsored by the individual NIH institutes. Our vision reflects what we want to achieve by working together: The Clinical Center will enhance its reputation as international model of excellence and innovation in the conduct of and training in clinical research. Three long-range goals top the list of what's most important for us to accomplish. They are excellence in clinical research, quality of patient care, and cost effectiveness and efficiency. We've developed a series of specific strategies to reach these goals and the board has asked us to work with the individual institutes to develop more. So far they include:
Your enthusiasm and innovative thinking are key elements to all that we need to do, so important that I've set aside money in this year's budget to recognize individual and team efforts supporting our projects and plans. Many current projects already have been developed to bolster these strategies.
We've opened a Guest House for patients and families. We have forged new
alliances in the extramural community. Our Core Course in Clinical Research
has been well received. Both the Patient Recruitment and Referral Center
and the Protocol Coordination Service Center are up and running. These are
just a few examples. You'll be reading more about the specifics of individual
projects in upcoming issues of CCNews. workingWhen bad weather or some other emergency make travel dangerous, the Office of Personnel Management has two new policies to cover it. One is the adjusted work dismissal policy that permits non-emergency employees to leave work early. The other is an adjusted home departure policy that lets workers leave their homes later than normal. Both new policies hinge on the worker's normal work or home departure times. Say a snowstorm or hurricane is approaching. OPM may decide that workers should leave the office three hours early. That means that non-emergency workers who normally leave at 5 p.m. would be dismissed at 2 p.m. This plan replaces the old residential zone dismissal policy, which NIH was not subject to. NIHers are subject to the new adjusted work dismissal policy. Under the adjusted home departure policy, OPM could announce that an adjusted home departure policy is in effect and that employees should leave home two hours later than normal, for example. The guy who leaves home at 7 a.m. wouldn't pull out until 9 a.m. An employee who normally leaves home at 8:30 a.m. would wait until 10:30 a.m. The number of hours to delay will vary depending on the situation. This new plan replaces the old delayed arrival policy, which directed everyone to arrive at a certain time-and also put folks on the road just when road crews needed not to have them there. Officials note that these new policies will also be in effect in cases of widespread power failures. Exceptions allow for immediate closures when necessary. Questions? Check with the Division of ICD Consulting in the NIH Office of Human Resource Management, 496-4491. briefs:Alter on panelA Clinical Center staffer is on the panel of experts expected to present during the March 24-26 NIH consensus development conference on management of hepatitis C. Dr. Harvey J. Alter, chief of the infectious diseases section in the Department of Transfusion Medicine, will discuss blood donors with Hepatitis C at 10 a.m. on March 24 in the Natcher Conference Center. After a day and a half of scientific presentations and audience discussions, an independent, non-federal consensus panel will weigh the scientific evidence and draft a statement to present to the attendees on March 26. It will address key questions about the disease, including its natural history, appropriate approaches to diagnosing and monitoring patients, and what to recommend to patients on preventing transmission. Summary of benefits comingInterested in knowing what your total compensation package contains? What do you pay for benefits? Which benefits are free? Watch for your individualized statement of benefits that will be mailed to your home in mid-March. It's provided by the Office of Human Resources Management and designed to provide an overview of your total compensation and summaries of your pay and benefits. It's simple, convenient, and can provide estimates for future financial planning. Call Sharon Reed or Mike Pometto, 496-6924, if you have questions or comments. FOCC sponsors spring fairPotters, weavers, dried floral arrangers, glass and jewelry makers, wood crafters, and fabric artists are among those who'll display their wares during the Friends of the Clinical Center (FOCC) spring craft fair on March 20 in the Visitors Information Center. The event is set for 9 a.m.-3 p.m. Each craftsperson has been asked to donate an item for raffle and tickets ($1 each or six for $5) will be sold outside the B1 cafeteria March 17-20. Winners will be able to select their own prize, planners note. The event benefits FOCC, a program that helps CC patients and their families facing financial emergencies while participating in medical research here. For more information on the spring fair, call Kai Lakeman, 530-7530. Symposium setThe science of brain disease, an NIH symposium set for March 18 in Masur Auditorium, will highlight the achievement and promise of neuroscience. Speakers will include Dr. Sangram Sisodia, Johns Hopkins School of Medicine; Dr. James McNamara, Duke University Medical Center; Dr. John Maunsell, Baylor College of Medicine; Dr. Susan McConnell, Stanford University; Dr. John Marler, NINDS; Dr. Nora Volkow, Brookhaven National Laboratory; Dr. Joseph Takahashi, Northwestern University; and Dr. Eric Kandel, Howard Hughes Medical Center. For details, call JoAnn Pass at 496-1752. Mason diesLong-time CC volunteer Pearl Mason died Jan. 6. Memorial services were held Jan 24 at St. James Episcopal Church in Potomac. A Red Cross volunteer for 30 years, she received special honors during a ceremony recognizing CC volunteers that was held last April. 
TouringIsrael's new ambassador to the U.S., Eliahu Ben-Elissar (left), recently toured the Clinical Center with Dr. John Gallin, CC director. He's one of the more than 1,400 visitors who tour the building with the special events section staff each year.  Overlooking historyWhen the Clinical Center opened its doors in 1953, a brushed aluminum shield and building name graced the north and south entrances. Both were removed-and almost forgotten-during construction projects during the 1970s and 1980s. Building Services recently rescued the signage from storage and had the words "Warren Grant Magnuson" faithfully fashioned to match the original "Clinical Center." The shield and building name are now in place over the front door. They'll move to the south entrance when that becomes the main door during construction of the new building. |
|
|